Speaking the Language
of the Brain
Dose with confidence by optimizing the volume and message of VNS Therapy™
![]()

Reach Target Stimulation Volume

The combination of output currents and pulse width comprises the ‘volume’ of critically important neural stimulation. Combined with the physical size and shape of the VNS Therapy™ electrode, they jointly determine the intensity of electrical stimulation–working in concert to activate vagus nerve fibers by way of the electrode-tissue interface.1
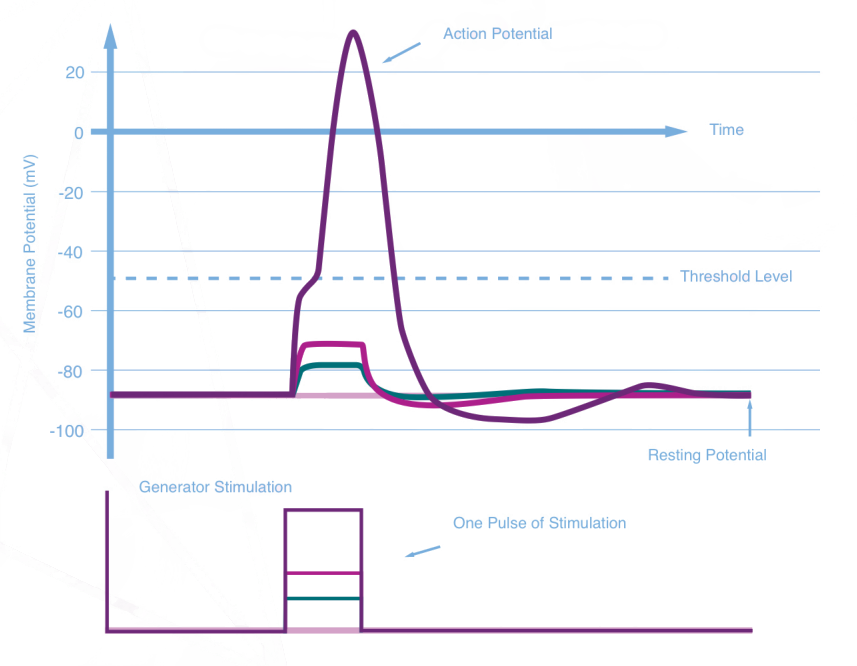
Achieving action potential is a
critical component
An action potential is only initiated when a charge density is strong enough to depolarize the nerve.3
Vagus Nerve Stimulation Threshold Strength-Duration Curve for Responders.
Output Current-Pulse Width Range4

The top line represents data from responders in the LivaNova E05 extension study and the VNS TherapyTM Registry. The curve in the middle is based on data collected by Evans et al. Because the study was conducted intraoperatively, it should be noted that the results may not fully represent the stimulation needed to recruit fibers as fibrosis develops.4
*Response is defined as a reduction in seizure frequency that is 50% or greater from baseline.
Getting the volume right increases response
Greater than 90% of patients who responded had output currents above 0.75 mA and 200 microseconds.4

Use signal frequency to send
the right therapeutic message
Signal frequency and duty cycle can be considered as the therapeutic neural modulation ‘message’ for VNS Therapy.1
The duty cycle defines the cadence of dose repetition of VNS Therapy™.2
Initial duty cycle = 10%–defined as2:

Increased duty cycle may improve efficacy*2
It provides greater repetition of the therapeutic message and may increase the likelihood of response. There is limited data on higher duty cycles, and higher duty cycles will affect battery life.1
A 16% duty cycle– defined as:

A 25% duty cycle– defined as:

Duty Cycle = (ON Time + 4 seconds) / (ON Time + OFF Time), for which ON and OFF Time are measured in seconds.
*As a safety precaution, duty cycles above 50%, even at lower frequencies, are highly discouraged.2

Target range settings deliver
the right message at the right volume1
Together, output current, pulse width, and signal frequency can be considered the dose of VNS Therapy™. Duty cycle can be regarded as dosing frequency.1
Patients implanted and dosed shortly after their initial drug-resistant epilepsy diagnosis were shown to benefit from VNS Therapy™. However, chronically underdosed patients currently on VNS Therapy™ may still benefit from target-range titration.1
Reach the Target Range
Faster titration to the target range = Earlier therapeutic responsePatients who were titrated to the target range within 3 months per the recommended protocol achieved onset of response faster1,2 |
Approximately 50% of VNS TherapyTM patients take longer than 1 year to reach target dosing1Consider the speed of titration, especially in light of evidence from a posthoc analysis supporting earlier therapeutic response to VNS TherapyTM when patients were titrated according to labeling recommendation compared to those who were not, often without an increase in rate and adverse events.3 |
Consider the target dose combination for DRE patients as1:
If using a pulse width of 500 microseconds at a signal frequency of 30 hertz, the output should be 1.5 milliamps. |
If using a pulse width of 250 microseconds at a signal frequency of 20 hertz, the output should be 1.75 milliamps. |
† Based on a retrospective analysis of VNS TherapyTM titration and dosing practice that compiled patient data from 12 clinical studies. The analysis included randomized controlled trials and open-label observational studies. Clinical response was defined as a reduction in seizure frequency from a baseline of 50% or greater.2
The most common stimulation-related adverse effects are2:

DYSPHONIA

PARESTHESIA
COUGH
DYSPNEA
Most side effects associated with VNS Therapy™, 2, 4, 5:
- Occur during stimulation and generally diminish over time
- May be diminished or eliminated by the adjustment of parameter settings
- May be controlled by use of the magnet
References 1. Data on file. LivaNova, USA 2022 2.VNS TherapyTM [VNS TherapyTM System Epilepsy Phyisican’s Manual US Version] Houston, TX; LivaNova USA; May 2020. 3. Fahoum F, Boffini M, Kann L, et al. VNS paramters for clinical response in epilepsy. Brain Stimul. 2022;(15):814-821. 4. Ben-Menachem E. J Clin Neurophysiol. 2001;18(5):415-418. 5. VNS TherapyTM [Patient’s Guide for Epilepsy] Houston, TX; LivaNova USA; April 20120

